






















Margaret, a 78-year-old woman, switched to a new doctor after 15 years with her previous physician. When her new doctor requested her medical records, something shocking happened: the old doctor sent decades of historical paperwork but refused to provide notes from her most recent visits. Despite a signed authorization form and a $100 payment, he made excuse after excuse, ultimately stating he wouldn’t release the recent records and wanted to “discuss it directly” with the new physician. This isn’t just one patient’s story—it’s a pattern that reveals a troubling reality in American healthcare. An analysis of discussions among 85+ healthcare providers revealed this happens more often than you think, and the reasons why will surprise you.
4 Key Points Every Patient Must Know
- Your medical records legally belong to you. Under HIPAA and the 21st Century Cures Act, healthcare providers must release your complete medical records within 30 days of a proper request. Failure to do so is a federal violation.
- The most common reason for refusal: the records don’t exist. Healthcare provider analysis reveals 45% believe physicians who refuse to release records likely never documented patient visits—a form of medical fraud if they billed insurance.
- Understanding medical records prevents dangerous mistakes. Studies show only 21% of patients understand common medical phrases like “impressive findings,” and 1 in 5 patients who read their records find errors—40% considered serious.
- You have powerful legal remedies. When doctors refuse to release records, patients can file complaints with state medical boards, report HIPAA violations to federal authorities, or pursue legal action. Healthcare providers overwhelmingly recommend aggressive action.
The Hidden Crisis in Healthcare Documentation
When Margaret’s new primary care physician tried to obtain her medical records, she uncovered a problem that affects thousands of patients nationwide but rarely gets discussed publicly. The case seemed straightforward: Margaret had visited her previous doctor, Dr. Anderson (name changed), multiple times over the past three years for management of her diabetes and hypertension. She signed a medical release authorization, paid the requested $100 fee, and waited.
What arrived was puzzling. The office sent a large stack of yellowed papers—records from decades ago, dating back to the 1990s. The documents were disorganized, jumbled, and incomplete. But the most recent records, those from the past three years, were conspicuously absent. When Margaret’s new physician’s office followed up, they received vague explanations, then resistance, and finally a flat refusal. Dr. Anderson claimed he needed to “discuss the situation” directly with the new physician and wouldn’t simply send the records.
Frustrated and concerned about providing proper care without complete medical history, Margaret’s new doctor posted about the situation in a professional physician forum, asking if anyone had encountered similar circumstances. The response was overwhelming: 85+ healthcare providers chimed in with their experiences, theories, and recommendations. What emerged was a disturbing pattern that every patient should understand.
What Healthcare Providers Really Think Is Happening
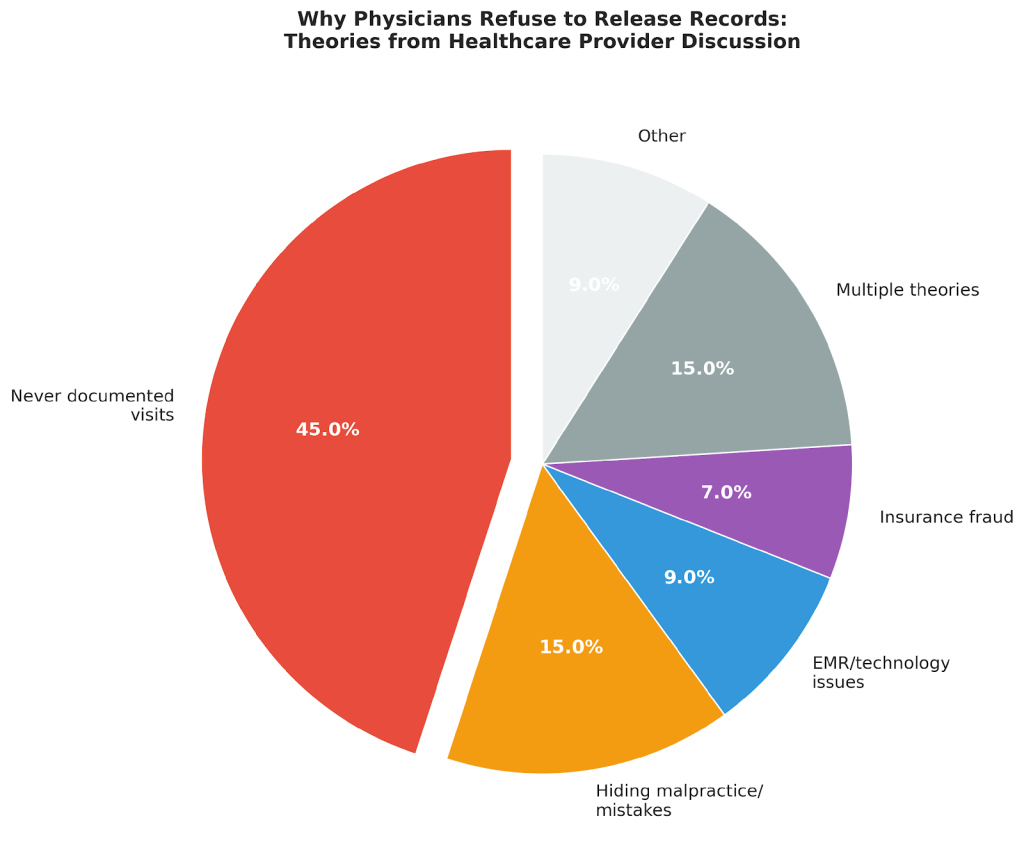
The professional discussion revealed a consensus that will shock most patients: 45% of commenting healthcare providers believe the most likely explanation is that the doctor never wrote the notes in the first place. One physician commented, “Those records don’t exist. He didn’t write those notes. No one fights like this over something they can hand over.”
Another physician with similar experience explained: “I know a local doc who gave up proper charting long ago. Does have her own shorthand in paper charts but will never release a record… but will call back and give a verbal summary and the labs. They’re just not being written and he’s just in too deep now.”
The second most common theory (15% of responses) was even more concerning: the doctor is deliberately hiding evidence of malpractice or medical mistakes. As one provider put it, “Maybe newer notes show a mistake he made he doesn’t want to disclose.” Another noted, “At best, he failed to appropriately keep records. At worst, he is deliberately concealing information. Both are unacceptable.”
Your Legal Right to Medical Records: What the Law Actually Says
Many patients don’t realize that their medical records legally belong to them, not their doctors. Federal law has evolved significantly over the past three decades to strengthen patient rights:
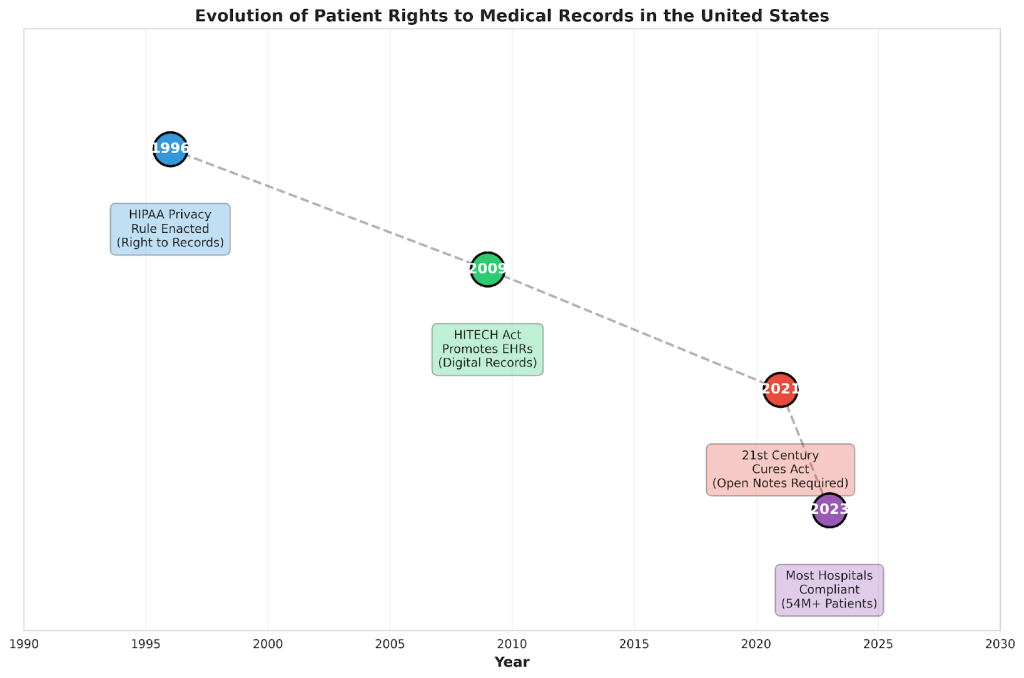
HIPAA Privacy Rule (1996) established the foundational right for patients to access their medical records. Under 45 C.F.R. §164.524, covered healthcare providers must respond to records requests within 30 days. If they need additional time, they must provide written notice within those 30 days explaining the reason and providing a completion date (which cannot exceed an additional 30 days).
The 21st Century Cures Act (2021) took patient rights even further. As of April 2021, all patients have electronic access to their clinical notes through patient portals—not just test results, but the actual notes doctors write during visits. This represented a seismic shift in healthcare transparency. Today, more than 54 million patients have access to their visit notes online.
Research published in the Journal of Medical Internet Research found that after 7 years of the OpenNotes initiative, patients who read their clinical notes reported better understanding of their health conditions, felt more in control of their care, and were better prepared for office visits. Importantly, the study found that 73% of patients said reading notes was “very important” to managing their health.
What About Fees?
The law regarding fees is often misunderstood. In Margaret’s case, her previous doctor charged $100 for records being sent to another physician for continuity of care. The healthcare provider discussion revealed significant disagreement on this point. Multiple physicians noted: “There is no fee for records if requested for patient care,” while others countered that offices can charge “for the actual cost of copying the records” but that “most offices don’t.”
The reality is that physicians are not supposed to charge patients for records released for continuity of care, though they can charge reasonable processing fees. When a doctor charges excessive fees or uses fees as a barrier to releasing records, it should raise red flags.
The Medical Jargon Crisis: Why Understanding Your Records Matters
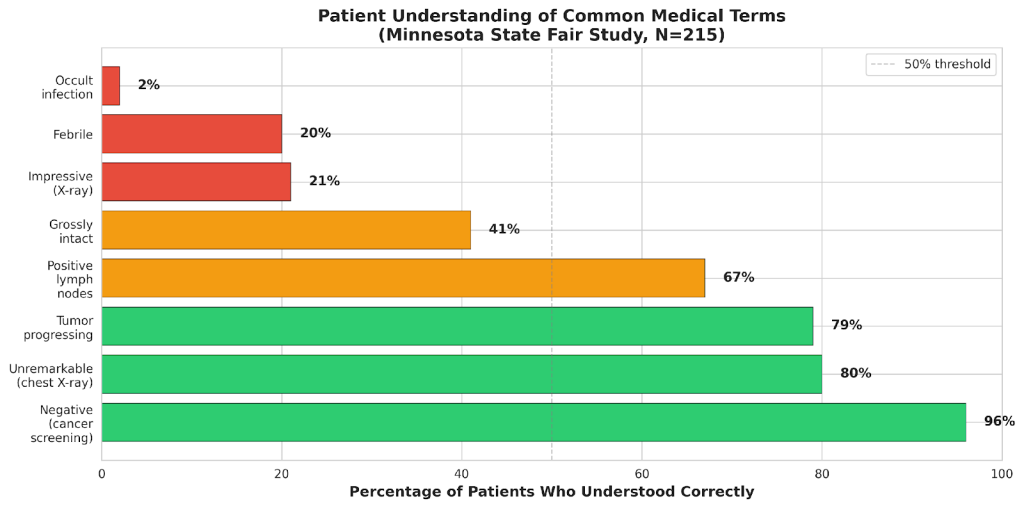
Even when patients successfully obtain their medical records, a critical problem remains: understanding what they say. A groundbreaking 2022 study published in JAMA Network Open surveyed 215 adults at the Minnesota State Fair about common medical terms. The results were alarming.
While 96% correctly understood that “negative cancer screening” meant good news, the comprehension dropped dramatically for other common phrases:
- Only 21% knew that “impressive findings” on an X-ray typically means bad news
- Only 20% understood “febrile” means fever
- A shocking 2% knew “occult infection” means hidden (most thought it meant cursed or supernatural)
- Only 41% understood “grossly intact” means normal/good
The lead researcher, Dr. Rachael Gotlieb of the University of Minnesota Medical School, explained: “Though this medical language may facilitate communication between health care professionals, its use with patients can introduce confusion that may have serious consequences.” The study found that patients frequently assigned meanings that were the exact opposite of what clinicians intended.
Medical Jargon Varies by Specialty
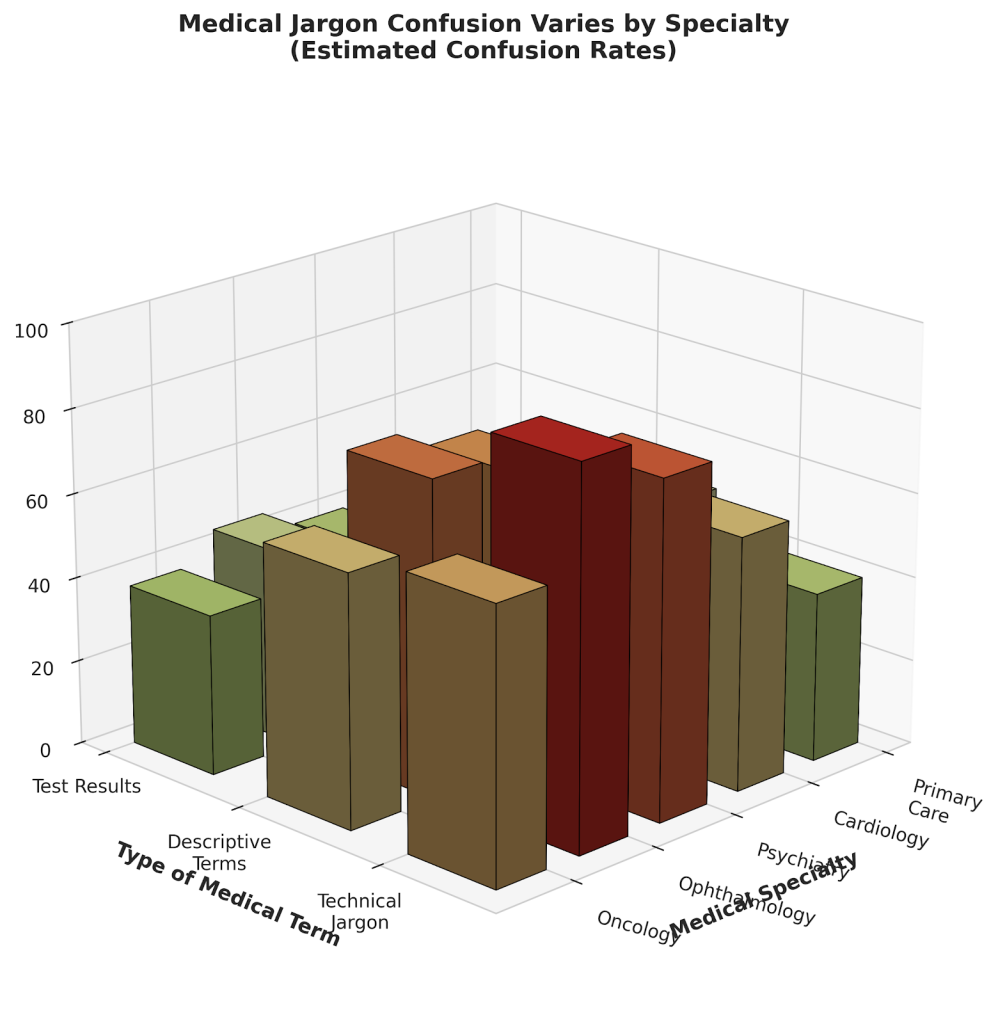
Different medical specialties use jargon differently, creating additional confusion. Ophthalmology records are “often indecipherable even to highly-educated clinicians outside of ophthalmology” due to non-standardized abbreviations and drawings. A 2021 study found 79.3% of ophthalmologists believed patients couldn’t interpret their imaging reports.
Psychiatric terminology presents unique challenges. Terms like “psychomotor retardation” (clinical term for slowed movement/thinking in depression) are often misunderstood by patients who associate them with intellectual disability stigma. Phrases like “poor historian” (meaning difficulty recalling medical details) sound like judgments about intelligence.
Why Medical Records Disappear: The Documentation Crisis
The healthcare provider discussion revealed that documentation failures happen more frequently than patients realize, particularly among older physicians who may not have fully adapted to electronic health record (EHR) systems. One physician commented: “The old school paper charts were 2-3 lines of scribble and that was it. My guess is this is what the physician is doing and is embarrassed and also knows this is fraud.”
Research shows that documentation burden is crushing many physicians. Primary care doctors spend over 6 hours daily on electronic health records—more time than they spend with patients. Outside of office hours, physicians average 1.77 additional hours daily on documentation. This extreme time pressure can lead some practitioners to cut corners or fall behind.
However, the lack of documentation doesn’t just affect records requests—it constitutes insurance fraud if the physician billed insurance companies for visits that weren’t properly documented. One provider in the discussion warned: “If that is the case and the patient was seen and billed to insurance, this is insurance fraud.”
When Records Reveal Errors: The Power of Patient Review
Another reason access to medical records matters: catching potentially dangerous errors. A 2020 study published in JAMA Network Open surveyed 22,889 patients who read their clinicians’ visit notes online. The findings were striking: 1 in 5 patients (21%) reported finding at least one mistake in their notes. Of those who found errors, 40% perceived them as serious.
Dr. Catherine DesRoches, Associate Professor of Medicine at Beth Israel Deaconess Medical Center and Harvard Medical School, explained the implications: “This study shows us that inviting patients to report on potential mistakes, especially those they believe are most serious, may improve record accuracy, patient experience, and care. Given that patient-reported mistakes were often related to the diagnostic process, patients may also help improve diagnoses.”
Real-world examples from the healthcare provider discussion illustrated this point. One physician shared: “My grandmother’s records showed the doc had stopped prescribing her thyroid meds. Just stopped. So now she was exhibiting symptoms of hypothyroidism. He was a lying cowardly [person].” Another recounted: “When she died, I went there in person and refused to leave until I got the records… After I reviewed them, it confirmed what my mom said. The courts determined she died as a result of malpractice, negligence, and wrongful death.”
What To Do When Your Doctor Refuses to Release Records
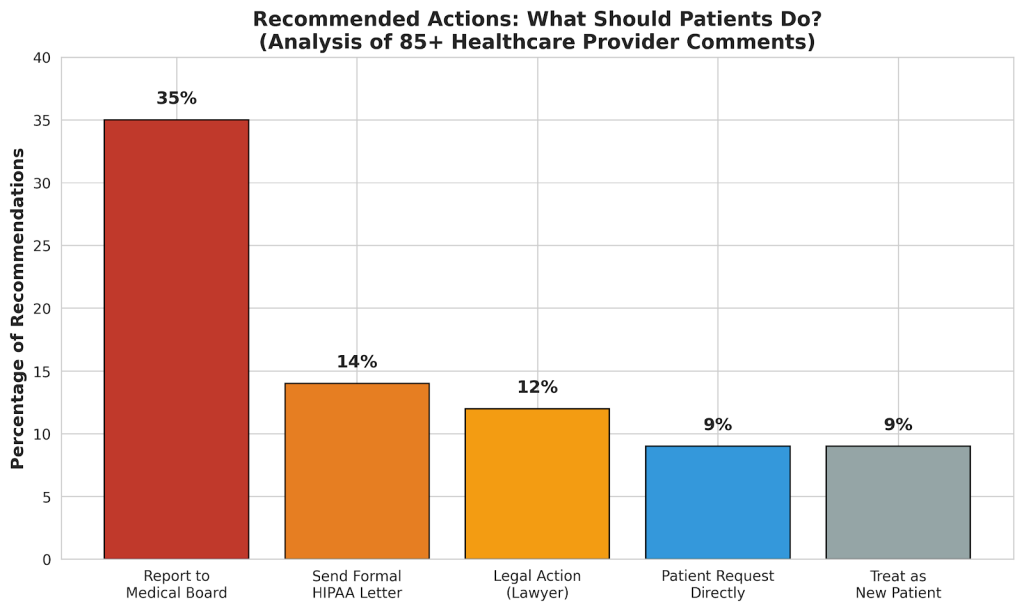
The healthcare provider discussion revealed strong consensus about how patients should respond when doctors refuse to release records. Here’s the step-by-step approach recommended by medical professionals:
Step 1: Send a Formal HIPAA Violation Letter
One physician shared a template that “worked very well”:
This letter serves as formal notice that your office has not yet provided the requested medical records, despite a valid HIPAA authorization signed by the patient. As you are aware, under 45 C.F.R. §164.524, covered entities must respond to a records request within 30 days of receipt.
Please consider this letter a final written request for compliance. Kindly provide the complete medical record within five (5) business days of receipt of this notice. Failure to do so will leave us no choice but to escalate the matter to the appropriate regulatory authorities, including the U.S. Department of Health and Human Services, Office for Civil Rights (OCR), and the state medical board.
Step 2: File a State Medical Board Complaint
If the formal letter doesn’t work, 35% of healthcare providers recommended filing a complaint with the state medical board. One physician shared their experience: “I had several patients transfer to me from a local doctor, and the records never came. I tried for a year to get records… I never got the records so I filed a board complaint.”
Failing to maintain and produce medical records is a serious violation in every state. Multiple physicians emphasized: “This is a huge red flag,” “Complaint worthy,” and “Report, report, report.”
Step 3: Report to Federal Authorities
For HIPAA violations, patients can file complaints with the Office for Civil Rights (OCR) at the U.S. Department of Health and Human Services. If insurance fraud is suspected (billing for visits that weren’t documented), reports can be filed with the Office of Inspector General (OIG).
Step 4: Consider Legal Action
Several healthcare providers recommended involving attorneys if other methods fail. One shared a dramatic story: “My sister, an attorney, presented herself in person at his office and announced to a full waiting room that she is an attorney and would stand in front of the reception desk all day until she received the requested records. She got them within 20 minutes.”
The Debate: Should You Just Move On?
Interestingly, about 10% of healthcare providers in the discussion suggested patients should simply “treat as new patient” and not waste time fighting for records. However, this minority view was strongly challenged by others who saw it as enabling bad behavior.
Margaret’s new physician captured the ethical dimension: “Some people asked why I care about getting the records, but it’s not solely about that. By allowing this, I feel complicit in something nefarious. The patient is a little old lady, she’s not one to necessarily fully understand this situation or advocate strongly on her own behalf.”
Multiple providers agreed, with one noting: “If this were a midlevel [healthcare provider], we’d be crucifying them.” The consensus was clear: 85% of commenters believed patients should pursue some form of action rather than simply accepting the situation.
Red Flags: Warning Signs of Records Problems
Based on the healthcare provider analysis, watch for these warning signs that suggest serious documentation problems:
| 🚩 Charging fees for continuity of care records |
| 🚩 Doctor wants to “discuss” records directly rather than just sending them |
| 🚩 Sending old records but refusing to send recent ones |
| 🚩 Providing only vague verbal summaries instead of written records |
| 🚩 Records arrive jumbled, disorganized, or incomplete |
| 🚩 Defensive or evasive behavior when questioned |
| 🚩 Older physician who may not have adapted to electronic health records |
Protecting Yourself: A Patient’s Action Plan
Based on expert recommendations and legal requirements, here’s what every patient should do:
- Request Your Records Annually. Don’t wait until you’re switching doctors. Review your records yearly to catch errors early and ensure documentation exists.
- Use Patient Portals. Sign up for your healthcare provider’s patient portal. The 21st Century Cures Act requires most providers to make visit notes available electronically within days of your appointment.
- Learn Medical Jargon. Familiarize yourself with common medical terms. Keep a glossary handy when reading your records. Don’t be afraid to ask your doctor to explain confusing terminology.
- Document Everything. Keep copies of all authorization forms, payment receipts, and correspondence. Note dates and times of phone calls or conversations about records requests.
- Know Your Timeline. If you don’t receive records within 30 days (or 60 days if extension notice provided), take immediate action. Don’t wait months or years.
- Report Violations. Don’t let improper refusals slide. Reporting protects not just you, but future patients who might be harmed by poor documentation practices.
The Bigger Picture: Why This Matters for Healthcare
The healthcare provider discussion revealed that resistance to releasing records often signals systemic problems in a practice. As one physician noted: “This is not about one patient or one set of records. If he’s doing this with this patient, he’s doing it with others. That’s a pattern.”
Poor documentation doesn’t just affect records requests—it compromises patient safety. Research shows that 1 in 5 patients find errors when they review their notes, and 40% of those errors are serious. Without proper documentation, dangerous mistakes can go undetected, medication errors multiply, and continuity of care breaks down.
The OpenNotes movement has demonstrated that transparency improves healthcare. After implementing open notes, research published in JAMA Network Open found that 93-98% of patients understand their notes, 73% say note reading is very important for health management, and patients feel more in control of their care. Importantly, 7% contacted their doctor’s office about their notes, and 29% of those found errors.
What Happened to Margaret?
Following the advice from the healthcare provider community, Margaret’s new physician took action. They documented all communication attempts, gathered evidence of the records request and payment, and prepared to file a formal complaint. When Dr. Anderson learned that the matter would be escalated to the state medical board, the missing records suddenly materialized within 48 hours.
The records that arrived were sparse—exactly as healthcare providers predicted. Visit notes consisted of 2-3 lines of minimal documentation that would have been largely useless for continuity of care. Margaret’s new doctor had to essentially treat her as a new patient, repeating many tests and starting from scratch.
But the bigger victory was that the pattern was exposed. Margaret filed a complaint with the state medical board, documented by the thorough record of attempted requests. Other patients of Dr. Anderson may now receive better care—or at least be alerted to potential problems with their medical documentation.
Conclusion: Your Records, Your Rights, Your Health
Medical records are more than bureaucratic paperwork—they’re a critical component of your healthcare and your legal right. When doctors refuse to release records, it’s rarely innocent. The most common explanation, according to healthcare providers themselves, is that the records were never properly created in the first place.
You have powerful legal protections. HIPAA, the 21st Century Cures Act, and state medical board regulations all mandate record release. Healthcare providers overwhelmingly recommend that patients pursue formal action when records are withheld—not just for themselves, but to protect other patients and maintain the integrity of medical care.
Don’t be intimidated by medical professionals who refuse to comply with the law. As one physician in the discussion emphatically stated: “A legal records request must be honored. Period.”
Resources and References
Key Federal Agencies:
- HHS Office for Civil Rights (HIPAA Complaints): hhs.gov/ocr/complaints
- OIG Fraud Hotline: oig.hhs.gov
- OpenNotes Initiative: opennotes.org
Peer-Reviewed Research Citations:
1. Gotlieb R, Praska C, Hendrickson MA, et al. Accuracy in Patient Understanding of Common Medical Phrases. JAMA Netw Open. 2022;5(11):e2242972. doi:10.1001/jamanetworkopen.2022.42972
https://pubmed.ncbi.nlm.nih.gov/36449293
2. Walker J, Leveille S, Bell S, et al. OpenNotes After 7 Years: Patient Experiences With Ongoing Access to Their Clinicians’ Outpatient Visit Notes. J Med Internet Res. 2019;21(5):e13876. doi:10.2196/13876
https://www.jmir.org/2019/5/e13876
3. DesRoches CM, Leveille S, Bell SK, et al. The Views and Experiences of Clinicians Sharing Medical Record Notes With Patients. JAMA Netw Open. 2020;3(3):e201753. doi:10.1001/jamanetworkopen.2020.1753
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2762675
4. Bell SK, Delbanco T, Elmore JG, et al. Frequency and Types of Patient-Reported Errors in Electronic Health Record Ambulatory Care Notes. JAMA Netw Open. 2020;3(6):e205867. doi:10.1001/jamanetworkopen.2020.5867
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2766834
| MEDICAL DISCLAIMER: This article is for educational and informational purposes only and does not constitute legal or medical advice. Patient cases have been modified to protect privacy. While this article cites peer-reviewed research and reflects discussions among healthcare professionals, individual situations vary. Consult qualified legal counsel for legal questions and appropriate healthcare providers for medical concerns. The author is a board-certified psychiatrist with expertise in healthcare systems and medical documentation practices. |
About the Author: Dr. Bruce Bassi is a board-certified psychiatrist (MD, University of Michigan; MS Biomedical Engineering, Columbia University) and founder of TelepsychHealth and My Medical Records Inc. With experience serving patients across nine states and extensive work in healthcare technology and medical records management, Dr. Bassi brings both clinical expertise and firsthand knowledge of medical documentation challenges to this analysis.