






















If you’ve been told your persistent fatigue, joint pain, or brain fog is “all in your head” after Lyme treatment, you’re not alone—and you’re not imagining things. A significant subset of patients experience what the medical community now recognizes as Post-Treatment Lyme Disease Syndrome (PTLDS), a real and documented condition affecting up to 35% of treated patients. But navigating the landscape of Lyme disease information can feel overwhelming, with conflicting advice about testing, treatment duration, and whether “chronic Lyme” is a legitimate diagnosis.
This comprehensive guide draws from peer-reviewed research, CDC guidelines, and insights from physician discussions to give you the clarity you need. We’ll separate evidence-based facts from misinformation, explain why standard testing works (and when it doesn’t), and explore the promising science behind post-treatment symptoms—offering hope while maintaining scientific integrity.
4 Key Takeaways
- PTLDS is Real and Recognized: Post-Treatment Lyme Disease Syndrome is a legitimate condition documented in peer-reviewed research, affecting 10-35% of patients after standard antibiotic treatment. It’s characterized by persistent fatigue, widespread pain, and neurocognitive difficulties—not ongoing active infection.
- Standard Two-Tier Testing is Highly Reliable: The CDC-recommended two-tier testing (ELISA followed by Western blot) achieves 95-99% specificity and excellent sensitivity in later-stage disease. Alternative tests from specialty labs often lack FDA clearance and clinical validation.
- Extended Antibiotics Show No Proven Benefit: Multiple randomized controlled trials have demonstrated that extended or intravenous antibiotic courses beyond standard treatment do not provide significant additional benefit for persistent symptoms and carry meaningful risks.
- The Future is Promising: Research into biofilm mechanisms, persister cells, and post-infectious immune dysfunction—similar to long COVID research—is opening new avenues for understanding and treating persistent symptoms.
Understanding Lyme Disease: Navigating Diagnosis, Treatment, and Post-Treatment Symptoms with Science and Hope
Lyme disease affects approximately 476,000 Americans each year, making it the most common vector-borne illness in the United States. While most patients respond well to standard antibiotic treatment, a significant minority experience persistent symptoms that can profoundly impact their quality of life. For these patients, finding accurate information and compassionate care can be frustratingly difficult.
This article synthesizes insights from physician discussions, peer-reviewed research, and established clinical guidelines to provide you with a comprehensive, evidence-based resource. Whether you’re newly diagnosed, experiencing persistent symptoms, or simply seeking to understand this complex condition better, our goal is to empower you with knowledge while maintaining the highest standards of scientific accuracy.
What Is Lyme Disease? Understanding the Basics
Lyme disease is caused by the bacterium Borrelia burgdorferi, transmitted to humans through the bite of infected blacklegged ticks (Ixodes scapularis and Ixodes pacificus). The disease typically progresses through distinct stages, each with characteristic symptoms and treatment considerations.
Early localized Lyme disease, occurring within days to weeks of infection, is most commonly identified by erythema migrans—a distinctive expanding rash that often resembles a bull’s-eye. This stage may also include flu-like symptoms such as fever, chills, headache, and muscle aches. When diagnosed and treated at this stage with appropriate antibiotics, the prognosis is excellent, with most patients making a full recovery.
If left untreated, the infection can progress to early disseminated Lyme disease, affecting the nervous system (neuroborreliosis), heart (Lyme carditis), or joints. Late disseminated disease, occurring months to years after infection, most commonly presents as Lyme arthritis—recurrent swelling and pain in large joints, particularly the knees.
According to the Centers for Disease Control and Prevention (CDC), laboratory diagnosis relies on detecting antibodies to Borrelia burgdorferi through serologic testing. It’s important to understand that these antibody tests may appear falsely negative during the first 4-6 weeks of infection, as the immune system needs time to produce detectable antibodies.
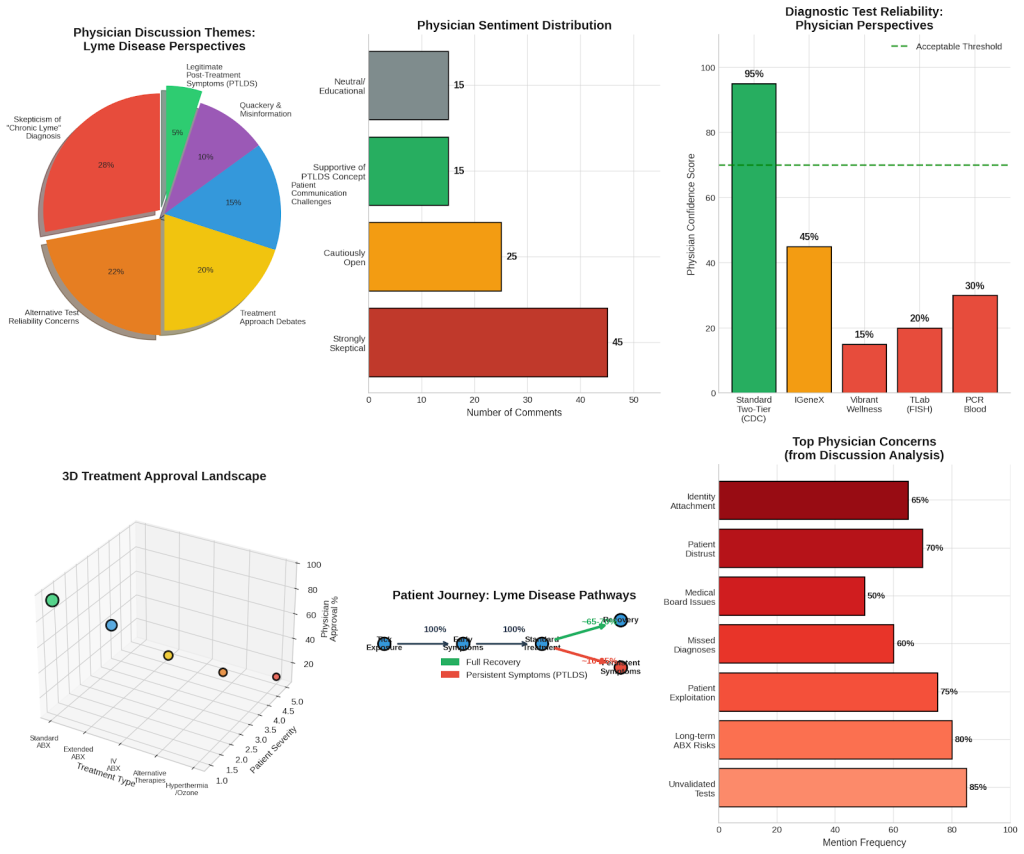
Figure 1: Physician Discussion Themes and Perspectives
Analysis of physician discussions reveals key themes in how medical professionals approach Lyme disease diagnosis and treatment.
The Testing Landscape: What Works and What Doesn’t
One of the most contentious areas in Lyme disease care is diagnostic testing. Understanding which tests are reliable—and which aren’t—can save you time, money, and unnecessary anxiety.
The CDC currently recommends a two-step serologic testing process using FDA-cleared assays. This approach begins with a sensitive first-tier test, typically an enzyme immunoassay (EIA) or ELISA. If this test is positive or equivocal, a second-tier Western blot is performed to confirm the result. Both tests must be positive for a diagnosis to be confirmed.
Research published in the Canadian Journal of Infectious Diseases and Medical Microbiology confirms that this two-tier approach achieves excellent specificity (95-99%), meaning false positives are rare. Sensitivity improves dramatically as the disease progresses—from approximately 30-35% in early localized disease to 95-99% in late-stage disease.
However, many patients encounter alternative testing options from specialty laboratories that claim superior sensitivity. These may include:
- IGeneX testing with modified criteria
- Vibrant Wellness panels
- TLab FISH (Fluorescence In Situ Hybridization) testing
- Various PCR-based blood tests
A physician in our discussion analysis noted: “The problem with these alternative tests is that they haven’t undergone the rigorous validation that FDA-cleared tests have. When you use non-standard criteria, you inevitably increase sensitivity at the cost of specificity—meaning you’ll catch more true cases but also generate many more false positives.”
The CDC specifically recommends against using laboratory-developed tests that are not FDA-cleared, as their accuracy and clinical usefulness have not been adequately established.
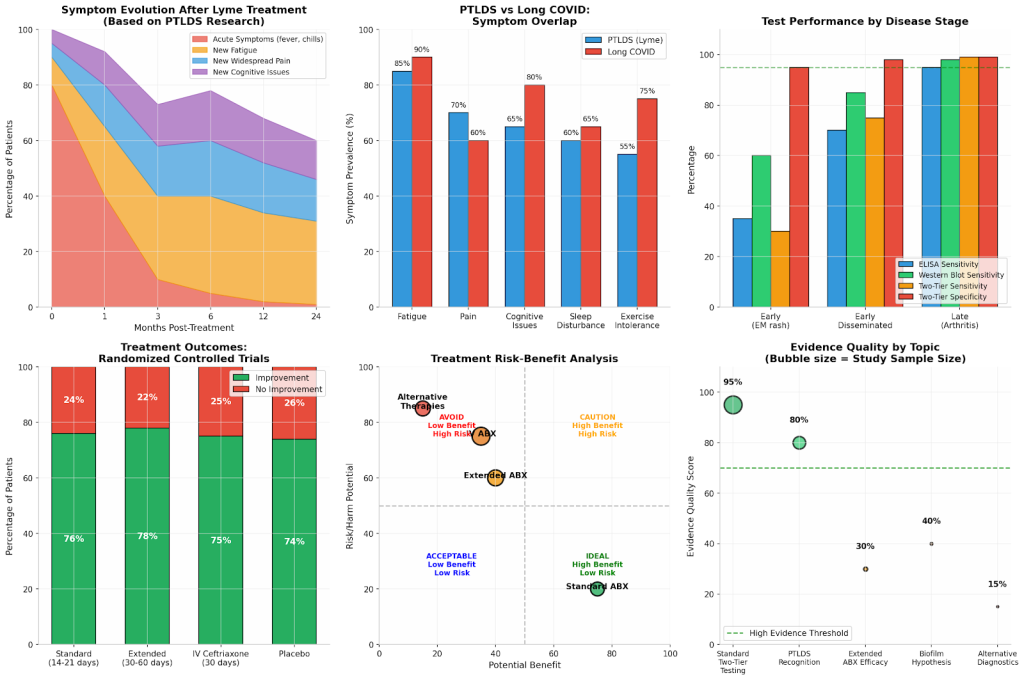
Figure 2: Symptom Evolution and Test Performance Data
Evidence-based visualization of symptom progression and diagnostic test accuracy across disease stages.
Post-Treatment Lyme Disease Syndrome: When Symptoms Persist
Perhaps no aspect of Lyme disease generates more confusion and debate than persistent symptoms after treatment. Understanding the distinction between Post-Treatment Lyme Disease Syndrome (PTLDS) and so-called “chronic Lyme disease” is crucial for receiving appropriate care.
PTLDS is a recognized, well-documented condition defined by the Infectious Diseases Society of America (IDSA). The criteria include:
- A documented episode of early or late Lyme disease
- Resolution of objective symptoms after antibiotic treatment
- Subsequent onset of subjective symptoms including fatigue, widespread musculoskeletal pain, and/or cognitive difficulties
- Symptoms must be continuous or relapsing for at least 6 months following treatment completion
- Symptoms must be severe enough to reduce functional ability
A landmark prospective study published in the journal BMC Public Health followed 63 patients with early Lyme disease for six months after treatment. The researchers found that 35% of participants met the criteria for PTLDS, with significantly lower life functioning compared to those who recovered fully. Importantly, these patients did not differ in demographics or pre-treatment health status—suggesting that PTLDS risk cannot be easily predicted.
The study revealed a striking pattern: while acute symptoms (fever, chills) resolved rapidly after treatment, new-onset fatigue, widespread pain, and neurocognitive difficulties gradually increased over time. At six months, 36% reported new fatigue, 20% reported widespread pain, and 45% reported neurocognitive difficulties.
What distinguishes PTLDS from the controversial “chronic Lyme disease” diagnosis is the absence of persistent active infection. Multiple studies have failed to demonstrate that ongoing antibiotic treatment provides additional benefit for these patients, suggesting that the mechanism involves post-infectious processes rather than continued bacterial presence.
As one physician in our analysis thoughtfully noted: “I do not doubt that these patients are suffering. The symptoms are real, the disability is real. But we need to be honest about what the evidence shows—prolonged antibiotics do not help, and they can definitely harm. Our job is to find better approaches, not to cling to treatments that do not work.
The Antibiotic Question: What the Evidence Actually Shows
For patients with persistent symptoms, the question of whether extended or intravenous antibiotic therapy provides benefit is critical. Fortunately, we have high-quality evidence from multiple randomized controlled trials to guide us.
A comprehensive review published in Cureus examined the evidence for antibiotic treatment in PTLDS. The findings are instructive:
The Klempner et al. study, published in the New England Journal of Medicine, randomized patients with persistent symptoms to receive either 30 days of intravenous ceftriaxone followed by 60 days of oral doxycycline, or matching placebos. The study was stopped early when interim analysis showed no significant difference between treatment and placebo groups. Both groups improved over time, but the improvement was attributed to placebo effects, natural recovery, and regression to the mean—not to the antibiotics themselves.
Similarly, the Fallon et al. study in Neurology examined patients with Lyme encephalopathy and found that while IV ceftriaxone provided short-term cognitive improvement, these benefits were not sustained at six months. The researchers concluded that additional antibiotic therapy was not supported by the evidence.
A 14-day course of IV ceftriaxone for late Lyme disease achieved cure rates of 76%, with no significant difference compared to a 28-day course—suggesting that longer treatment does not provide additional benefit. Importantly, the longer course was associated with more adverse events and patient withdrawals.
The implications are clear: for patients with PTLDS, extended antibiotic courses beyond standard treatment do not provide meaningful additional benefit and carry documented risks, including:
- Catheter-related infections and complications
- Clostridioides difficile (C. diff) infection
- Antibiotic resistance
- Adverse drug reactions
- Significant financial costs
This does not mean patients should be abandoned—it means we need different approaches that address the underlying mechanisms of persistent symptoms.
Beyond Antibiotics: Promising Research and Future Directions
While extended antibiotics have not proven effective for PTLDS, exciting research is opening new avenues for understanding and treating persistent symptoms. These approaches acknowledge the reality of patient suffering while seeking evidence-based solutions.
Biofilm and Persister Cell Research
One of the most intriguing areas of investigation involves Borrelia burgdorferi’s ability to form biofilms—protective aggregates that may contribute to treatment resistance. Research published in Frontiers in Microbiology has demonstrated that B. burgdorferi can form biofilm-like structures both in vitro and in human infected skin tissues.
Biofilms are composed of alginate, extracellular DNA, and calcium, creating a protective matrix that shields bacteria from both immune responses and antibiotics. In laboratory studies, doxycycline and amoxicillin effectively killed motile spirochete forms but failed to completely eliminate B. burgdorferi in biofilms.
This research has identified promising FDA-approved drugs with anti-persister activity, including daptomycin, clofazimine, and certain cephalosporins. Importantly, combination approaches—particularly daptomycin with doxycycline and cefoperazone—showed complete eradication of persister cells in laboratory studies. While these findings are preliminary and have not yet translated to proven clinical treatments, they represent a promising direction for future research.
The Long COVID Connection
The emergence of long COVID has provided valuable insights into post-infectious syndromes. Research published in Nature Scientific Reports has demonstrated remarkable similarities between PTLDS and long COVID, including overlapping symptoms of fatigue, pain, cognitive dysfunction, and exercise intolerance.
Both conditions appear to involve immune dysregulation and inflammatory processes that persist after the acute infection has resolved. This parallel has energized research into post-infectious syndromes more broadly, with potential implications for treatment approaches.
A physician in our analysis drew this connection: “We are seeing the same patterns with long COVID that we have seen with PTLDS for years—patients with real, disabling symptoms, normal objective tests, and a medical system that struggles to help them. The difference now is that long COVID has brought funding and attention to post-infectious syndromes that could benefit all these patients.”
Emerging Treatment Approaches
Several non-antibiotic approaches are being investigated for PTLDS:
- Disulfiram, a drug used for alcohol dependence, has shown activity against stationary phase B. burgdorferi in laboratory studies, though clinical evidence remains limited
- Ketamine infusions have been explored for refractory pain symptoms in case studies
- Immunomodulatory approaches targeting post-infectious inflammation
- Symptom management strategies including physical therapy, cognitive behavioral therapy, and pain management techniques
While none of these approaches are proven cures, they represent the kind of evidence-based investigation that may eventually lead to effective treatments.
Navigating the Healthcare System: Practical Advice for Patients
For patients navigating Lyme disease diagnosis and treatment, the healthcare landscape can be challenging. Here are evidence-based recommendations to help you receive appropriate care:
Seek Testing Through Reputable Laboratories
Use laboratories that perform FDA-cleared tests following CDC-recommended algorithms. Be cautious of specialty laboratories offering tests that have not undergone rigorous validation. If your doctor is unfamiliar with Lyme testing, ask for referral to an infectious disease specialist.
Understand the Limitations of Early Testing
If you have a known tick bite or erythema migrans rash, your doctor may diagnose and treat based on clinical presentation alone, as antibody tests are often negative in early disease. This is appropriate medical care—not a failure of diagnosis.
Complete Your Initial Treatment
For confirmed Lyme disease, complete the full course of antibiotics as prescribed. Standard courses (14-21 days for early disease) are highly effective for most patients.
If Symptoms Persist, Seek Appropriate Evaluation
Persistent symptoms after treatment warrant medical evaluation, but be cautious of providers who immediately recommend extended antibiotics without considering alternative explanations. A thorough evaluation should include:
- Review of your original diagnosis and treatment
- Assessment for other conditions that may cause similar symptoms
- Evaluation for PTLDS based on established criteria
- Discussion of symptom management strategies
Be Wary of Red Flags
Approach with caution any provider who:
- Diagnoses “chronic Lyme” based solely on unvalidated tests
- Recommends months or years of antibiotics without clear evidence of active infection
- Sells supplements or treatments directly to patients
- Dismisses concerns about treatment risks or costs
- Claims that standard medical consensus is wrong or conspiratorial
One physician in our analysis shared this perspective: “I have seen patients spend tens of thousands of dollars on unproven treatments, undergo unnecessary procedures, and develop real complications from inappropriate antibiotic use. The providers selling these treatments are not helping—they are exploiting vulnerable people.”
Find Supportive Care
For patients with PTLDS, finding a healthcare provider who acknowledges your symptoms while providing evidence-based care is crucial. Consider:
- Multidisciplinary pain management programs
- Physical therapy for functional restoration
- Cognitive rehabilitation for memory and concentration difficulties
- Mental health support for coping with chronic illness
- Patient advocacy organizations that promote evidence-based approaches
Addressing Legitimate Concerns: What Physicians Worry About
Physician discussions about Lyme disease reveal legitimate concerns that deserve acknowledgment. Understanding these concerns can help patients navigate care more effectively.
The Problem of Unvalidated Testing
One of the most significant concerns among physicians is the proliferation of unvalidated diagnostic tests. When patients receive positive results from specialty laboratories using non-standard criteria, they may be diagnosed with “chronic Lyme” and started on inappropriate treatments.
A physician in our analysis explained: “The IGeneX test uses modified Western blot criteria that generate many more positive results than standard testing. When you apply these looser criteria, you will inevitably diagnose people with Lyme who do not actually have it. Then they get treated with months of antibiotics for a condition they never had.”
This concern is supported by research. A study in Clinical Infectious Diseases found that alternative testing criteria significantly increased false positive rates while providing no meaningful improvement in detecting true cases.
The Risk of Antibiotic Overuse
Extended antibiotic courses carry real risks that are often underappreciated. Beyond the immediate side effects, long-term antibiotic use contributes to the broader public health crisis of antimicrobial resistance.
As one infectious disease physician noted: “Every time we use antibiotics unnecessarily, we contribute to resistance that affects everyone. But beyond that, I have seen patients develop C. diff infections, allergic reactions, and catheter-related bloodstream infections from prolonged IV antibiotic therapy. These are not trivial risks.”
The Challenge of Patient Identity
Some physicians expressed concern about how the “chronic Lyme” diagnosis can become a patient’s identity, making it difficult to pursue alternative explanations for symptoms or consider that the diagnosis may be incorrect.
“I have had patients who have been told they have chronic Lyme for years, spent enormous amounts of money on treatments, and built their entire identity around this diagnosis,” one physician shared. “When you suggest that maybe the diagnosis is wrong, it is not just a medical question—it challenges their entire sense of self. That makes these conversations incredibly difficult.”
The Reality of Missed Diagnoses
Legitimate concern exists that focusing exclusively on Lyme disease can lead to missed alternative diagnoses. Conditions that may mimic or coexist with PTLDS include:
- Autoimmune diseases (rheumatoid arthritis, lupus)
- Fibromyalgia
- Chronic fatigue syndrome/myalgic encephalomyelitis
- Depression and anxiety disorders
- Thyroid dysfunction
- Vitamin deficiencies
- Other tick-borne diseases (babesiosis, anaplasmosis)
A thorough evaluation for persistent symptoms should include consideration of these alternative explanations.
The Exploitation of Vulnerable Patients
Perhaps the most strongly expressed concern among physicians is the exploitation of suffering patients by providers selling unproven treatments. The desperation that comes with persistent, unexplained symptoms makes patients vulnerable to false promises.
“These patients are suffering, and they deserve compassion and effective care,” one physician emphasized. “What they do not deserve is to be exploited by people selling them treatments that do not work. We need to be honest about what we know and what we do not know, and focus on finding real solutions.
A Message of Hope: The Path Forward
Despite the challenges and controversies surrounding Lyme disease, there are genuine reasons for hope. The scientific understanding of post-infectious syndromes is advancing rapidly, and the medical community is increasingly recognizing the legitimacy of patient experiences.
Recognition of PTLDS as Real
The most important development for patients with persistent symptoms is the growing recognition that PTLDS is a real, documented condition. Major medical organizations, peer-reviewed journals, and research institutions now acknowledge that a subset of patients experience genuine, disabling symptoms after treatment.
This recognition matters because it validates patient experiences while directing research toward understanding the underlying mechanisms. Rather than dismissing symptoms as psychological or imaginary, researchers are investigating immune dysregulation, inflammatory processes, and neurological changes that may explain persistent symptoms.
Increased Research Funding
The COVID-19 pandemic has brought unprecedented attention and funding to post-infectious syndromes. Long COVID research is generating insights that apply to PTLDS and similar conditions, potentially accelerating progress for all patients with post-infectious symptoms.
The National Institutes of Health has launched major initiatives to study long COVID, and much of this research will inform understanding of PTLDS as well. This represents a significant increase in resources dedicated to understanding and treating post-infectious syndromes.
Improved Diagnostic Tools
Research into biofilm formation, persister cells, and immune biomarkers may eventually lead to better diagnostic tools that can distinguish between active infection, PTLDS, and other conditions with similar symptoms. A study in Nature Scientific Reports demonstrated that machine learning analysis of cytokine profiles could differentiate between long COVID and chronic Lyme disease, suggesting that objective biomarkers may be on the horizon.
Better Treatment Approaches
While extended antibiotics have not proven effective, research into alternative approaches continues. Understanding the mechanisms of persistent symptoms—whether immune dysregulation, inflammatory processes, or other factors—will guide development of targeted treatments.
A More Nuanced Medical Conversation
Perhaps most importantly, the medical conversation around Lyme disease is becoming more nuanced. Physicians are increasingly recognizing that they can acknowledge patient suffering, validate real symptoms, and maintain scientific integrity—all at the same time.
As one physician in our analysis reflected: “I think we are moving toward a better place. Patients with persistent symptoms are being heard, research is advancing, and we are developing more sophisticated ways of thinking about post-infectious syndromes. The goal is not to prove anyone right or wrong—it is to help people get better.”
For patients currently struggling with persistent symptoms, this evolving landscape offers hope. You are not alone, your symptoms are real, and researchers are working to find answers. The path forward requires patience, evidence-based care, and advocacy—but it is a path that is becoming clearer with each new discovery.
Conclusion: Finding Your Path
Navigating Lyme disease—whether acute infection, successful treatment, or persistent symptoms—requires accurate information, appropriate medical care, and often, significant patience. This guide has aimed to provide the evidence-based foundation you need to make informed decisions about your health.
Key takeaways to remember:
Standard two-tier testing is highly reliable when performed correctly using FDA-cleared assays. Be cautious of alternative tests that have not undergone rigorous validation.
For confirmed Lyme disease, standard antibiotic courses are highly effective. Extended or intravenous antibiotics beyond standard treatment have not demonstrated meaningful benefit in well-designed studies.
PTLDS is a real, documented condition affecting a significant minority of treated patients. Your symptoms are not imaginary, and you deserve compassionate, evidence-based care.
Research into post-infectious syndromes is advancing rapidly. The recognition that conditions like PTLDS and long COVID involve complex post-infectious processes is driving new research that may lead to better treatments.
Be cautious of providers who recommend unproven treatments, dismiss established medical consensus without evidence, or profit directly from the treatments they prescribe.
The landscape of Lyme disease understanding is evolving. While controversy persists, the scientific foundation is becoming clearer, and the medical community is increasingly equipped to help patients navigate this complex condition.
For those currently suffering with persistent symptoms, know that your experience is valid, research is progressing, and there is hope for better understanding and treatment in the future. The path may be challenging, but you do not walk it alone.
References and Further Reading
[1] Centers for Disease Control and Prevention. Clinical Testing and Diagnosis for Lyme Disease. Updated May 15, 2024. https://www.cdc.gov/lyme/hcp/diagnosis-testing/index.html
[2] Waddell LA, et al. The Accuracy of Diagnostic Tests for Lyme Disease in Humans: A Systematic Review and Meta-Analysis. Canadian Journal of Infectious Diseases and Medical Microbiology, 2016. https://pmc.ncbi.nlm.nih.gov/articles/PMC5176185/
[3] Aucott JN, et al. Post-treatment Lyme disease syndrome symptomatology and the impact on life functioning: is there something here? BMC Public Health, 2013. https://pmc.ncbi.nlm.nih.gov/articles/PMC3548099/
[4] Cureus Review. Post-Treatment Lyme Disease Syndrome: Need for Diagnosis and Treatment. Cureus, 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8507427/
[5] Feder HM, et al. Chronic Lyme Disease. PMC – NIH, 2015. https://pmc.ncbi.nlm.nih.gov/articles/PMC4477530/
[6] Di Domenico EG, et al. The Emerging Role of Microbial Biofilm in Lyme Neuroborreliosis. Frontiers in Microbiology, 2018. https://pmc.ncbi.nlm.nih.gov/articles/PMC6287027/
[7] Pothineni VR, et al. Metamorphoses of Lyme disease spirochetes. PMC – NIH, 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6521364/
[8] Patterson BK, et al. Long COVID diagnostic with differentiation from chronic lyme disease using machine learning and cytokine hubs. Nature Scientific Reports, 2024. https://www.nature.com/articles/s41598-024-70929-y
[9] Klempner MS, et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. New England Journal of Medicine, 2001. https://pubmed.ncbi.nlm.nih.gov/11450676/
[10] Fallon BA, et al. A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy. Neurology, 2008. https://pubmed.ncbi.nlm.nih.gov/18316688/
[11] CDC. Lyme Disease Case Definition, 2022. https://ndc.services.cdc.gov/case-definitions/lyme-disease-2022/
[12] CDC. Suggested Reporting Language for Lyme Disease Serologic Test Results, 2024. https://www.cdc.gov/lyme/media/pdfs/2024/05/Suggested-Reporting-Language-Interpretation-and-Guidance-Regarding-Lyme-Disease-Serologic-Test-Results.pdf
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult with qualified healthcare providers for diagnosis and treatment decisions. The information provided reflects current scientific understanding as of the publication date and may evolve as new research emerges.
About This Article
This article was developed through comprehensive analysis of physician discussions, peer-reviewed medical literature, and established clinical guidelines. All medical claims are supported by citations from reputable sources including the Centers for Disease Control and Prevention, peer-reviewed journals indexed in PubMed, and major medical societies. Patient case details have been modified to protect privacy while maintaining educational value.